Megaloblastic anaemia is caused by deficiency of folate or cobalamin (Vit B12). The peripheral blood is sometimes characterised by pancytopenia and an increased mean corpuscular volume (MCV).
Pathophysiology:
- Haematopoietic cells undergo apoptosis due to intracellular folate or vitamin B12 deficiency. Since the deficiency of the latter causes folate trap and folate cannot be utilised, this results in increased uracil mis-incorporation into DNA and increased p53 and p21 proteins.
- The erythroblasts that survive this apoptotic process give rise to larger than normal reticulocytes (macrocytes).
Peripheral smear may show pancytopenia. Ovalomacrocytes, usually with considerable anisopoikilocytosis, is the main feature.
Mean corpuscular volume (MCV) is more than 100 fl. In others, MCV may be normal due to excessive fragmentation of red cells. Polychromatophilic cells are reduced.
Reticulocyte count may be less than 1%. The leucocyte count is reduced due to reduction in the number of neutrophils and lymphocytes.
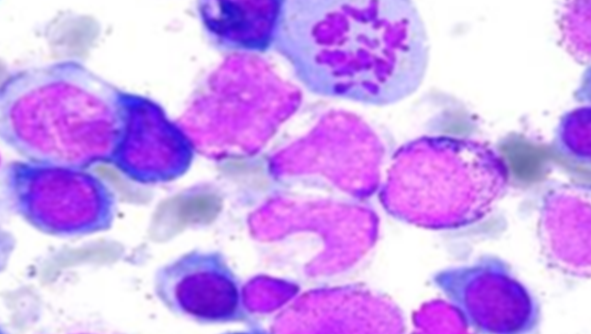
Hypersegmented neutrophils are usually seen. A minimum of five percent of five lobed or a single six lobed neutrophil is considered significant.
Thrombocytes are reduced in number, but rarely cause hemorrhagic complications. Macrocytosis and hypersegmented neutrophils occurring together strongly suggests megaloblastic haematopoiesis.
Bone marrow
Megaloblast is a designation first applied by Ehrlich to the abnormal erythrocyte precursors found in the bone marrow of patients with pernicious anemia. These are known to be the morphologic expressions of a biochemical abnormality and retarded DNA synthesis.
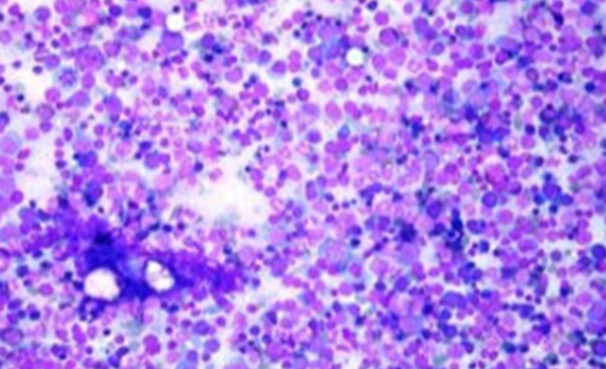
The aspirate is hypercellular. The M: E ratio is normal or reduced and there is an accumulation of primitive cells due to selective death of more mature forms. The most characteristic finding is dissociation between nuclear and cytoplasmic development in the erythroblasts, with the nucleus maintaining a primitive appearance despite maturation and hemoglobinization of the cytoplasm.
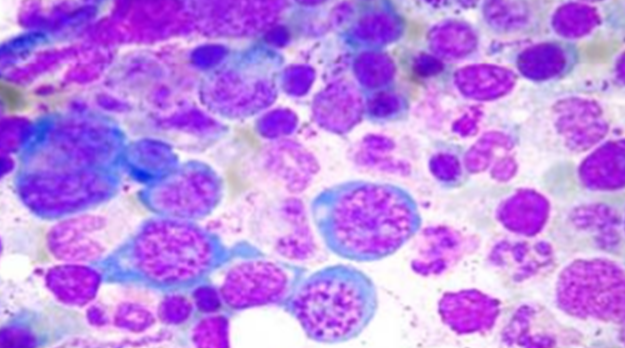
Fully hemoglobinized (orthochromatic) erythroblasts, which retain the nuclei, may beseen. The nucleus of the megaloblast has an open, fine and lacy appearance: the cells are larger than normoblasts and an increased number of cells with eccentric lobulated nuclei or nuclear fragments may be present. Mitoses and dying cells are more frequent than normal.
Giant and abnormally shaped metamyelocytes and enlarged hyperpolypoid megakaryocytes are characteristic.
Treatment: Vit B12 and Folic acid replacement
In indians most common anemia is megaloblastic anaemia due to neutritional deficiency. So neutrition should be proper. Take vit b12 rich diet like Non vegiterian foods only source of vit b12.